CHICAGO – Counties in Southern and Appalachian states have some of the highest incidence rates of diabetes, while counties in large metropolitan areas reported some of the highest numbers of new cases, a government study looking at diabetes incidence rates across the United States revealed.
"We’re hoping that people can use these data to identify high-risk areas, and use it as a tool in implementing and developing diabetes prevention interventions," said Nilka R. Burrows, an epidemiologist at the Centers for Disease Control and Prevention, who presented her abstract at the annual scientific sessions of the American Diabetes Association.
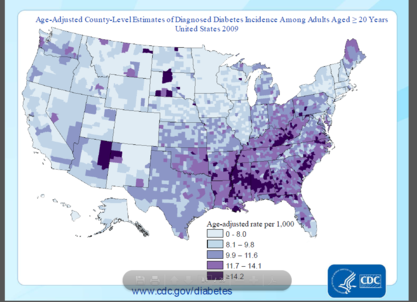 Courtesy of the CDC
Courtesy of the CDC
Because changes in incidence rates are one of the first indicators of whether diabetes prevention efforts have been successful, the county-level estimates can help local policy makers, she said.
The interactive maps of diabetes incidence can be found at www.cdc.gov/diabetes/atlas.
Although the study is one of the first of its kind, "the findings don’t tell us anything we didn’t know," said Mercedes R. Carnethon, Ph.D., associate professor at Northwestern University, Chicago, who was not involved in the study. "But [the study] really serves to reemphasize how substantial the burden of the problem is in the high-risk areas," she said.
 Naseem S. Miller/IMNG Medical Media
Naseem S. Miller/IMNG Medical Media
Nilka R Burrows
In 2010, nearly 26 million Americans had diabetes, and 2 million were diagnosed within the past year, said Ms. Burrows.
The authors looked at data for the period of 2004-2009 for adults aged 20 years or older in 3,143 U.S. counties or county equivalents, to identify geographic patterns and high-risk areas.
The county-level incidence estimates incorporated data from the Behavioral Risk Factor Surveillance System (BRFSS) and the U.S. Census.
The sample was age-adjusted to the 2000 U.S. standard population, Ms. Burrows said.
In 2009, the age-adjusted diabetes rate ranged from 4 per 1000 in Colorado to 21 per 1000 in Alabama. Areas that had high diabetes incidence rates (11.7 and higher) were mostly concentrated in Southern and Appalachian states, and in some counties in Arizona, New Mexico, Oklahoma, South Dakota, and Maine, Ms. Burrows reported.
The authors also looked for areas where there were more than 9,000 new diabetes cases in 2009. They identified several major metropolitan areas, including Los Angeles’ LA County with 50,000 new cases, Chicago’s Cook County with 30,000 new cases, Harris County in Houston, and Maricopa County in Phoenix, with 20,000 new cases each.
Urban counties with higher numbers of cases didn’t coincide with counties in rural areas that had the highest incidence rates, since absolute numbers are a function of population size, said Ms. Burrows.
The data "highlighted where we have the highest burden of the problem," said Dr. Carnethon. "So when you think about resources to manage diabetes, including clinical resources, such as people being in those locations, clinicians in particular, we obviously have a higher need for practitioners to deal with diabetes in those parts of the U.S."
The study also showed that the number of counties with a diabetes incidence rate of 11.7 or higher increased from 500 (16%) in 2004 to 870 (28%) in 2009. The median incidence rate was 9.7 in 2004, and 10.1 in 2009.
When calculating the 2009-to-2004 ratio of county-level diabetes incidence rates, the ratios ranged from 0.65 in Indiana to 1.79 in Pennsylvania.
Using a liberal confidence level of 0.1, the 2009-to-2004 incidence rates didn’t change in most of the counties during the 5-year period.
The analysis has some limitations. The diabetes incidence may be underestimated because it was self-reported. Also, the estimates are subject to sampling variability. In addition, during a short time period of 5 years, incidence is not likely to change dramatically, and more years of data are needed.
Ms. Burrows said that surveillance of the information should continue to gauge diabetes prevention efforts.
Ms. Burrows and Dr. Carnethon had no disclosures.
nmiller@frontlinemedcom.com On Twitter @NaseemSMiller